AIDS is one of the most important and tragic problems that arose before all of humanity at the end of the 20th century. Acquired immune deficiency syndrome (AIDS) is a disease of viral etiology that affects the immune and nervous systems and is manifested by the development of severe infectious lesions and malignant neoplasms. AIDS is a complex scientific problem. The fight against AIDS is greatly complicated by the lack of effective therapeutic drugs, as well as the inability to vaccinate. That is why health education, complete and objective information to the general public about the relevance of the AIDS problem and effective ways to prevent infection are of crucial importance in the fight against the AIDS epidemic. The World Health Organization also pays major attention to health education work.
The first cases of infection were observed in Africa back in 1959, in the USA - since 1977. Since 1987, the spread of a new infectious disease has taken on the character of an epidemic. The disease is now registered in 152 countries around the world. Currently, the World Health Organization has registered about 2 million cases of AIDS. Data on the number of HIV-infected people, depending on the source, vary from 13 to 20 million, but at least 8 million of them are in Africa alone. According to authoritative forecasts, in 2000 there will be from 40 to 110 million HIV-infected people in the world. AIDS is a difficult disease to control due to:
1) lack of effective treatments;
2) lack of means of primary prevention (vaccination);
3) difficulties in contacting the population groups most affected by AIDS. Experts believe it will take 8 to 20 years to create a vaccine. The disease is characterized by a high mortality rate - 40 - 90%. In all the time that has passed since the first cases of AIDS were described, there has not been a single fact of cure or recovery from this disease. All carriers of the AIDS pathogen are potentially sick. Virological studies carried out by Luc Montagnier's scientific groups at the Pasteur Institute
(France) and Robert Gallo at the National Cancer Institute (USA) made it possible in 1983 to discover the real cause of AIDS - T-lymphotropic retrovirus, which later received the name HIV - hyman immunodeficiency virus (HIV - human immunodeficiency virus).
Doctors already have about two hundred thousand case histories, so the clinical features of AIDS have now been studied quite well. The most difficult thing to recognize is the disease at the very beginning. When the disease process goes far, the patient experiences three main types of disorders (unfortunately, they can be present simultaneously in various combinations, causing a particularly severe course of the disease). First of all, more than half of the patients experience various secondary infections caused by bacteria, fungi, viruses or even protozoa. This is candidiasis of the mucous membranes of the oral cavity (“thrush”) or the esophagus, pneumocystis or herpetic pneumonia, cryptosporidial or cytomegalovirus lesions of the small or large intestine, tuberculosis of various organs and systems. More than half of the patients also experience neurological and mental disorders caused by damage to the central and peripheral nervous systems (the cause of these lesions is both HIV itself and its “allies” - cryptococci, toxoplasma, herpes simplex and herpes zoster viruses, etc. ). Finally, every third AIDS patient develops various tumors - sarcomas, gliomas, lymphomas, melanomas and other “...omas”.
From an epidemiological point of view, AIDS is an infectious disease of an anthroponotic nature with contact and vertical transmission mechanisms. The source of infection is an infected person at any stage of the disease, i.e., regardless of the clinical signs of the disease. The most intense transmission of the virus occurs through sexual contact with patients and virus carriers. The risk of infection during homosexual contacts is especially high, which can be explained by three reasons:
1) During homosexual contact, the pathogen with seminal fluid penetrates directly into the bed of the sexual partner through microtraumas in the mucous membrane of the intestine and anal canal. Taking into account the abundant venous blood supply to the rectum, the risk of infection of a passive partner seems high. The risk of infecting an active partner through erosions and cracks in the skin of the penis is quite high.
2) The rectal epithelium, due to the presence on the surface of its cells of the receptor protein CD 4, with which the gp 120 virus directly interacts, is capable of serving as a reservoir of the AIDS virus and thereby ensuring hematogenous dissemination of the pathogen in the body of a passive partner, even in the absence of microtraumas of the rectal mucosa, as well as infection active partner in the mechanism specified above.
3) Langerhas cells - macrophages of the rectal mucosa, carrying the CD 4 receptor protein on the surface and, as a result, having the ability to interact with HIV, after infection and migration from the regtal mucosa, they populate the stroma of lymph nodes of various locations, turning into other cellular elements of the microphage series. By contacting T4 lymphocytes in the lymph nodes, transformed microphages infect them and contribute to the dissemination of the AIDS pathogen in the body (Fig. 1).
Another important factor in HIV transmission is infected blood and its components. Infection occurs through transfusions of blood, plasma, drugs VIII or IX of coagulation factors. HIV can be transmitted through contaminated injection needles, syringes and other equipment.
The vertical mechanism of transmission of the pathogen (from mother to fetus) is carried out transplacentally or during childbirth.
In accordance with the described routes and factors of transmission of the pathogen, epidemiological analysis allows us to identify several groups at increased risk of AIDS:
1. Homosexuals and bisexuals. In the USA, where the number of AIDS patients today is the largest compared to other countries in the world, 73.6% of patients fall into this group.
2. Drug addicts who use intravenous drugs. Among AIDS patients registered in the USA, the proportion of this category of patients is 17%.
3.Prostitutes. Infection in this group reaches 40%, and in African countries - up to 90%.
4.Patients with hemophelia and persons occasionally exposed to transfusions of blood or its components. Research by French specialists (Sultan Y., 1987) shows that HIV infection in hemophilia patients in France reaches 48%, while in the USA more than 2/3 of patients are infected with the AIDS virus (Levine P.H., 1987).
5. Patients with syphilis and viral hepatitis B with a prolonged and chronic course. The epidemiological and partly pathogenetic connection between syphilis and AIDS is so significant that a number of researchers even consider AIDS as an opportunistic infection in patients with syphilis.
Regarding the epidemiological relationship between viral hepatitis and AIDS, the following has been established:
a) about 90% of patients with viral hepatitis B registered by the Center for Disease Control (USA) belong to the above risk groups for AIDS;
b) the exponential nature of spread in viral hepatitis B and AIDS are very similar;
c) about 80% of AIDS patients have serological markers of infection with the hepatitis B virus.
In recent years, it has been established that there is a connection between viral hepatitis B and AIDS, due not only to the general routes and factors of transmission of the pathogen, but also to much more fundamental mechanisms. It was found out (Noonan C., 1985; Jerom B., 1986) that in the genome of both pathogens there are regions characterized by significant similarity in nucleotide composition.
6. Children of mothers infected with HIV. Children of seropositive mothers become infected transplacentally or during childbirth in 75–90% of cases.
Considering the ways and factors of transmission of the AIDS virus, it is necessary to emphasize that the transmission of HIV is through contact and everyday life: through handshakes, hugs, kisses, through household items, dishes, etc. - is impossible. There is no reliable data on the transmission of HIV through transmission - through blood-sucking arthropods (mosquitoes, mosquitoes, ticks, etc.).
HIV belongs to the family of retroviruses, i.e. viruses, the genome of which (HIV with RNA) can be integrated into human genes, for example, into the genome of blood cells - lymphocytes - or brain cells.
The retrovirus owes its name to an unusual enzyme - reverse transcriptase, which is encoded in their genome and allows the synthesis of DNA on an RNA matrix. Thus, HIV is capable of producing DNA copies of its genome in host cells, such as “helper” T4 lymphocytes. Viral DNA is incorporated into the genome of lymphocytes, where its expression creates conditions for the development of chronic infection. DNA is integrated into the genetic apparatus of the cell and changes its vital activity, as a result of which viral proteins begin to form in this cell. These “bricks” then form into solid viral particles, which come out and penetrate other, not yet infected cells. The parent cell soon dies. The fact of HIV integration into the genome of the host cell will prove to be a very difficult obstacle to overcome for the development of antiviral agents that would not only suppress the infection, but also destroy it.
Immunodeficiency viruses are very small - from 70 to 100 thousand viral particles can fit on a line 1 cm long. HIV has a surface membrane typical of all retroviruses and contains a characteristic nucleoid (core part) of a rod-shaped or conical shape (Fig. 2). Three types of proteins have been identified in the core of the virion: p 24, p 18 and p 15 with molecular weights of 24, 18 and 15 kilodaltons, which have pronounced antigenic properties. Using immunoelectron microscopy, it has been established that protein p 18 is adjacent to the inside of the virus shell, p 24 forms a layer directly covering the core structures, and p 15 binds to RNA molecules. The virion core contains two RNA molecules and reverse transcriptase (Fig. 3). The virus envelope contains the glycoprotein gp 160, consisting of an epimembrane part designated gp 120 and a transmembrane part gp 41. The amino acid composition of gp 120 is quite variable. This explains the fact that last years the antigenic properties of HIV changed by 30% (Fig. 4).
The genome of the AIDS virus contains about 9200 nucleotides forming 9 genes, which are limited by long circular repeats on both sides of the seminucleotide chain. The genetic structure of HIV is characterized by the presence of three structural genes and six regulatory genes. Having penetrated the human body at the time of infection, this virus does not manifest itself in any way at the beginning, but only “adapts” and spreads to various organs and tissues. The so-called incubation (hidden) period of HIV infection continues for several weeks. At this time, the person is already infected, but it is still practically impossible to detect the infection. Then, the infected person often (but not always) develops an acute stage of HIV infection, which occurs as a “flu-like illness.”
The HIV life cycle includes a number of sequential stages (Fig. 5). At the first stage, a specific interaction of the envelope proteins of the gp 120 virus with the receptor proteins of the target cell occurs. Then the viral particles are captured by the cell by endocytosis and are released from the membrane in the cytoplasm (the “undressing” stage). It is likely that the activation of HIV proteins by cell protein kinases plays a fundamental role in the penetration of the virus into the cell. After this stage, DNA is synthesized using a viral RNA template using reverse transcriptase. Molecules of newly formed virus-specific DNA take on a ring-like shape (circularization) and migrate from the cytoplasm to the nucleus, where they are integrated (integration) into the genome of the affected cell. Part of the virus-specific DNA remains in the cytoplasm for a long time, not being integrated with the DNA of the host cell. Expression of viral genes ultimately leads to the production of virus-specific RNA and proteins, which determines the subsequent assembly of new virions “budding” from the surface of the infected cell.
Currently, there are three known pathogens of AIDS: HIV-1, HIV-2, HIV-3. HIV-1 (described above) causes the disease mainly in North Africa and Europe. In 1986, employees of the Pasteur Institute isolated another variant of the AIDS causative agent - HIV 2 - from patients in West Africa. It is much more similar to the monkey immunodeficiency virus. Today, the prevalence of HIV 2 among AIDS patients and virus carriers is 0.2%. In 1988, HIV-3 was detected from AIDS patients living in South Africa.
The antigenic composition of HIV 2 differs from that of HIV 1. The surface epimemdral glycoprotein has a slightly lower molecular weight than gp 120 and is designated gp 105. Nevertheless, gp 105 exhibits the same pronounced affinity for the receptor proteins of the target cell. Among the core proteins of HIV 2, proteins p 26 and p 16, which have antigenic properties, have been identified.
The genome of HIV 2 is slightly larger than HIV 1, and has 9671 nucleotides. The genome structure of the 2 identified AIDS pathogens is based on general principle, except that the regulatory gene vpx of HIV 2 differs in its characteristics from the vif gene, which is located in an almost similar region of HIV 1 RNA. It is believed that HIV 2 is characterized by a less pronounced infectious property, and the process caused by this virus is a longer duration of asymptomatic carriage than HIV 1 infection. Both HIV 2 and HIV 1 are characterized by relatively low resistance to physical environmental factors and the effects of the most common disinfectants. Under the influence of 0.5% calcium hypochlorite solution, 50 - 70% ethyl alcohol solution, the virus is inactivated within a few seconds. However, HIV is relatively resistant to ultraviolet and x-ray radiation.
The fact of the close connection of the pathogenic effect of HIV with the high affinity of the envelope structures of the virus to the components of the receptor apparatus of immunocompetent cells seems absolutely unambiguous. It is the affinity of the viral membrane glycoprotein gp120 (gp105- in the case of HIV-2) to the cellular receptor, designated CD4, that makes it possible for HIV to infect target cells. Taking into account exactly what types of cells carry the CD4 receptor on the cytoplasmic membrane, it becomes obvious that the target cells for the AIDS pathogen are: T-helper lymphocytes, macrophages and monocytes. Among non-immunocompetent cellular elements, CD4 carriers and, therefore, HIV reservoirs can be considered astrocytes-glial cells of the central nervous system, epithelial cells of the rectal mucosa and vascular endothelium (Ward J. M. et al., 1987). At the same time, the earliest stage in the development of HIV infection is the defeat of helper/inducer T-lymphocytes (CD4+ lymphocytes). The until now seemingly unambiguous opinion that after attachment (adhesion) of the gp120 envelope protein to CD4 on the T-helper/inducer membrane, passive endocytosis of the viral particle occurs, today can be supplemented and corrected. It has been shown (Weber J. N., Weiss R. A., 1988) that the previously described glycoprotein gp41 plays an extremely significant role in the penetration of HIV into the target cell. Researchers believe that after virus adhesion, the resulting supramolecular complex (gp120 (gp105)-CD4) shifts, freeing up a zone on the T-helper/inducer membrane for contact with gp41. The latter, “screwing” into the plasma membrane of the affected cell, modifies its properties in such a way that the subsequent penetration of the virion into the cell is greatly facilitated. This is confirmed by the results of studies of the influence of monoclonal antibodies to gp41 on the interaction of HIV with target cells in vitro, according to which these antibodies almost completely prevented the fusion of the virus with the cell. The data obtained will likely be used to create a vaccine against the AIDS virus.
It has been convincingly shown (Kulberg A. Ya., 1988) that in the structure of the gp120 molecule there are areas that are very similar in composition and, therefore, antigenic properties to certain areas of the extracellular parts of the receptors for protein and polypeptide hormones. The degree of homology between the amino acid composition of gp120 and these receptor proteins reaches 40-45%. When analyzing the amino acid sequences in the conserved zones of HLA antigens (leukocyte histocompatibility antigens) class II and the envelope proteins of 13 HIV isolates, homology was revealed between the N-terminal domain of the HLA-DR and HLA-DQ antigens (amino acids 19-25) and the C-terminal domain of the gp41 protein ( amino acids 838-844) (Golding H. et al., 1988). Thus, both surface glycoproteins of HIV, gp120 and gp41, are inducers of autoimmune reactions in patients with AIDS.
A significant addition to the characterization of the mechanisms of autoimmune processes against the background of HIV infection are the results of studies by Stricker R. B. et al. (1987), according to which the perverted production of antibodies under these conditions is also directed against polymorphic HLA-DR antigens found on the surface of Langerhans cells of the mucous membranes.
Summarizing the analysis of the role of auto-aggressive mechanisms in the formation of immunodeficiency in patients with HIV infection, it is appropriate to cite the conclusion of Professor Luc Montagnier, one of the discoverers of the AIDS virus: AIDS is more likely to be based on an autoimmune process with the effects directed towards T-helper lymphocytes, rather than the direct cytopathic effect of HIV (Montagnier L., 1987).
However, the direct cytopathic effect of the virus becomes increasingly significant with the progressive depletion of the CD4+ cell subpopulation, which for a long time remains a phenomenon of autoimmune origin.
In addition to accelerating the death of CD4+ lymphocytes, HIV disrupts the process of recognition of infected T-helper/inducer cells by cells that control the size of the cell population infected with any viruses. We are talking about the fraction of T-suppressor/cytotoxic lymphocytes that carry the CD8 receptor on their plasma membrane. These CD8+ lymphocytes recognize cells infected with viruses by “recognizing” virus-induced antigens on their surface. However, an indispensable condition for such recognition must be the presence on the surface of the infected cell, along with virus-induced antigens, of the so-called proteins of the major histocompatibility complex class I (MHC I). These proteins are present on the cytoplasmic membrane of all cells with a nucleus. Having identified the named membrane antigens, CD8+ lymphocytes destroy cells affected by the virus (Fig. 7).
Unlike the causative agents of other viral infections, HIV apparently encodes the synthesis of MHC I proteins with an altered structure that CD8+ lymphocytes are not able to recognize. As a result, lysis of infected CD4+ cells by T-cytotoxic lymphocytes does not occur, despite the presence of virus-induced antigens on their plasma membrane.
To a certain extent, the destruction of infected CD4+ lymphocytes still takes place, but it is probably realized in a different way. If there are adherent virions on the surface of CD4+ cells and if there are antibodies to HIV in the bloodstream, such cells are destroyed by lymphocytes - effectors of antibody-dependent cellular cytotoxicity. This hypothesis was confirmed in clinical observations of patients with hemophilia - carriers of HIV (Ekert H., 1987).
However, such a mechanism for eliminating infected cells, despite the compensatory nature and sanogenic orientation, makes a negative contribution to the development of depletion of the CD4+ lymphocyte subpopulation, which plays a central role in ensuring the functions of cellular immunity. Indeed, CD4+ lymphocytes, on the one hand, recognize antigens on the surface of antigen-presenting cells; on the other hand, through direct intercellular contacts and through the secretion of lymphokines (interleukin-2, interferon gamma), they ensure cooperation of immunocompetent cells in the dynamics of the immune reaction. Taking into account the above, it becomes clear why the depletion of the number of CD4+ cells and the formation of their functional inferiority leads to such a multifaceted imbalance and, ultimately, to a deficiency of the immune response.
It must be emphasized that in the early stages of HIV infection, when there is no significant decrease in the number of CD4+ cells, violations of the regulatory functions of T-helper/inducer cells play a special role in the development of an imbalance in the immune system. This is confirmed by the results of studies by Harper M.E. (1986), according to which the proportion of infected CD4+ lymphocytes does not exceed 0.01% of their number. Another explanation for this apparent contradiction between the extremely small number of infected lymphocytes and the pronounced picture of immunodeficiency can be data on the secretion by infected cells of a “soluble suppression factor” of a protein nature, possibly a component of the HIV envelope. The soluble suppression factor significantly disrupts the coordination interactions of CD4+ cells with other lymphocyte subpopulations.
The results of the work of Cheynier R. et al deserve the closest attention. (1988), according to which HIV-1 is also able to actively replicate in CD8+ lymphocytes (T-suppressor/cytotoxic cells) in vitro. If HIV replication in CD8+ cells occurs in vivo, then one could assume that subsequent inactivation of the T-suppressor subset by the virus is a significant additional factor contributing to the development of an autoimmune reaction in HIV-infected individuals. On the other hand, this phenomenon could explain the seemingly surprising fact that some AIDS patients experience depletion of the peripheral pool of both T-helper and T-suppressor cells
Another important mechanism of disruption of functional contacts between CD4+ cells and lymphocytes of other subclasses is the failure of CD4+ lymphocytes to recognize HIV antigens provided by specialized cells. It must be recalled that the process of identification by CD4+ lymphocytes of any antigens appearing on the surface of antigen-presenting cells (for example, macrophages) is possible only if there is another type of antigen-protein of the major histocompatibility complex class II (MHC II) on the plasma membrane of the latter. Possessing receptors for MHC II proteins, antigen-recognizing CD4+ lymphocytes simultaneously identify both the foreign antigen and MHC II proteins, and only in this case their reactive proliferation occurs and an immune response is formed (Fig. 8).
Infection of macrophages with the AIDS virus is accompanied by a violation of CD4+ - dependent recognition of HIV antigens: on the one hand, the macrophage ceases to express MHC II proteins on its surface, on the other, the receptor of the CD4+ lymphocyte infected with HIV is modified so that even MHC proteins appearing on the plasma membrane of the macrophage II are not recognized. In both cases, CD4+ lymphocytes do not perceive information from antigen-presenting macrophages.
It must also be emphasized that the affinity of the MHC II proteins of macrophages for the CD4 receptors on the surface of T-helper/inducer cells, which underlies the processes of antigen presentation by macrophages to T-helper/inducer cells, turns out to be as close as the affinity of gp120 for the named receptor formation. That is why gp120, expressed by infected cells, competes with MHC II proteins for CD4 receptors and thus disrupts the processes of macrophage-lymphocyte cooperation.
The above does not exhaust the entire spectrum of dysfunctions of the mononuclear magocyte system in AIDS. Monocytes and macrophages of patients are characterized by reduced bactericidal and fungicidal activity and the ability to chemotaxis, as well as decreased functions of receptors for the Fc fragments of immunoglobulins. The defectiveness of Fc receptors is due to the blockade of a significant proportion of them by circulating immune complexes, as well as a decrease in the intensity of receptor recycling. The listed disorders largely explain the reason for the decrease in the activity of inflammatory reactions in AIDS patients.
The functional viability of subclasses of immunocompetent cells that have the cytotoxic properties of natural killer cells, natural killer cells, and T - cytotoxic cells is clearly reduced. The mechanisms of this phenomenon have not been fully established (Fig. 9).
The B-immune system is also affected during HIV infection. One of the most characteristic signs of B-cell dysfunction is their polyclonal activation, leading to the development of hypergammaglobulinemia (polyclonal gammopathy). The content of immunoglobulins of all classes increases, but especially of classes A and G in the blood serum. The level of immunoglobulins in the serum increases as HIV infection progresses, starting from the latent period, and reaches a maximum at the stage of the AIDS-associated symptom complex. In the stage of advanced AIDS, the content of immunoglobulins decreases significantly, with the exception of IgA, the level of which continues to increase. A number of studies suggest that it may be due to the reactivation of latent B-lymphotropic viruses, such as the Epstein-Barr virus, the degree of biological activity of which is controlled by T lymphocytes.
Despite the fact that the total concentration of serum immunoglobulins in conditions of HIV infection appears to be increased, patients have a characteristic disproportion in the levels of immunoglobulin subclasses, for example IgG. Thus, it has been shown that the content of IgG 1 and IgG 3 in such patients is increased, while the concentration of IgG 2 and IgG 4 is significantly reduced. A progressive decrease in IgG 2 levels may explain the increasing susceptibility of patients with HIV infection to the pathogenic effects of microorganisms such as Haemophilus, Pneumococcus and Staphylococcus aureus. Moreover, despite an increase in the number of circulating B lymphocytes that spontaneously secrete antibodies, these cells remain relatively refractory to the action of mitogens (for example, the mitogen of the monkweed), and also have an extremely weak response to neoantigens. Thus, despite hypergammaglobulinemia, the functional state of the B-immunity system in patients with HIV infection is similar to that against the background of severe hypogammaglobulinemia.
AIDS is a disease manifested by a deficiency of the immune system. The latter term refers to a set of mechanisms that provide protection to the body from bacteria, viruses, pathogenic fungi and other foreign agents. To perform a protective function in the human body, there is an immune system, which includes the thymus (thymus gland), bone marrow, lymph nodes, spleen and other tissues.
The most important cells of the immune system are lymphocytes, macrophages and monocytes. They have receptors that perceive HIV. Lymphocytes - the main cells of the immune system - are divided into T-lymphocytes and B-lymphocytes. T-lymphocytes, in turn, are divided into T-helpers and T-suppressors. HIV primarily affects T helper cells and to a lesser extent
degree macrophages. Neuroglial cells (nervous system) are also very sensitive to the causative agent of AIDS. HIV can directly infect hepatocytes (liver cells), cardiocytes (heart cells), other cells, and even bone tissue.
The interaction between the virus and the cells of the human body is due to the presence of special protein structures - so-called receptors. A viral receptor is a region of the virus that determines the “affinity” of the virus and a certain cell. A cell receptor is a section of the cell membrane, the molecular structure of which is characterized by selective affinity for certain molecules (viral receptors) and the ability to interact with them. Many cells of the human body (T-lymphocytes, macrophages, neuroglial cells and some others) have a special envelope protein CD 4, which interacts with the viral envelope antigen, bypassed by gp 120. The viral glycoprotein gp 120 “fits” CD 4 like a key to a lock. The interaction of CD 4 and gp 120 leads to the attachment of HIV to the cell and the subsequent penetration of the virus into it.
Macrophages are phagocytes, i.e. cells that capture microbes and other foreign antigens. Macrophages are distinguished between mobile (blood cells and monocytes) and non-motile, fixed in different tissues. Macrophages are found in almost all tissues, even in the brain. Therefore, macrophages are called “ubiquitous” cells. Macrophages are the first to recognize foreign agents that have entered the body, including HIV. Macrophages, like T-lymphocytes - helpers, have CD4 receptors, which enable HIV to attach to macrophages and penetrate the cell. The “ubiquitous” macrophages contribute to HIV infection of the entire body. True, there are not many CD4 marker molecules on the surface of macrophages, unlike T-hepers. In addition, HIV, although it damages macrophages, does not destroy them. Macrophages damaged by the AIDS virus recognize foreign agents much worse and “digest” them poorly.
T helper/inducer cells carrying CD 4 have been collectively called the “conductor of the immunological orchestra” and play a central role in the development of the immune response. These genes respond to contact with antigen by dividing and producing lymphokines such as interleukin-2, interferons and growth and differentiation factors of B lymphocytes. These lymphokines act as local hormones that control the growth and maturation of other types of lymphocytes, particularly cytotoxic/suppressor (CD 8) T lymphocytes and antibody-producing B lymphocytes. In addition, lymphokines influence the maturation and function of monocytes and tissue macrophages.
After infection, antibody production is initially unimpaired; the appearance of antibodies to the envelope and core proteins of the virus at this time even serves as the main sign of infection. Then the concentration of immunoglobulins of all classes in the serum increases, which indicates polyclonal activation of B lymphocytes. The reason for this is not entirely clear, but one can think that there is a direct activation of B lymphocytes by the virus. In later stages of the disease, the concentration of immunoglabulins tends to decrease.
The strongest impact of HIV is on the immune response mediated by T cells. As with other viral infections, the number of CD 8 cytotoxic suppressor cells may increase in the first days or weeks after infection. However, in healthy seropositive patients, the levels of lymphocytes and various subsets of T cells may remain normal. However, even at this stage, tests indicate a decrease in the proliferative response to control antigens (eg, tetanus toxoid or purified protein derivatives). Apparently, this is due to low production of interlikin 2. A person can have antibodies to HIV for a long time (i.e., sero-positive) and yet remain healthy. And yet, the number of CD 4 helpers/inducers is steadily falling, which, along with the appearance of new clinical symptoms, indicates the progression of the disease. Later, with a clearly expressed clinical picture, the number of CD 8 lymphocytes also decreases
Lymph node biopsy reveals many enlarged follicles in patients with lymphadenopathy, often infiltrated by CD 8 lymphocytes with cell depletion. At later stages, when the size of the lymph nodes returns to normal, the follicles appear to be “burnt out,” their normal structure is lost, and there are fewer and fewer cells.
According to the simplest assumption, the cause of immune deficiency may be the destruction of T helper/inducer cells by the virus, and probably also monocytes and macrophages. Another possibility is that the viral envelope glycoprotein that binds to CD 4 is involved in the interaction of helper/inducer cells with other cell types, which would block their normal activity. It has also been suggested that an autoimmune response may play some role in immunosuppression. In patients, along with lymphopenia, neutropenia, anemia or thrombocytopenia are sometimes observed, and these phenomena were explained by the production of autoimmune antibodies. There is no convincing data on the formation of such antibodies yet, although immune complexes have been found in the serum of patients. However, these are viral antigens and antibodies to them.
It is possible that infected CD 4+ - lymphocytes serve as targets for immune cytotoxic CD 4 + - T cells. But if this is so, then we are probably talking not about an autoimmune reaction, but about a protective reaction, since the destruction of virus-infected cells is a normal function of cytotoxic T lymphocytes. However, if cytotoxic T cells actually kill CD 4+ cells in this case, this should have a detrimental effect on the immune system.
AIDS - indicator diseases of group 1:
Candidiasis of the esophagus, trachea, bronchus and lungs.
Extrapulmonary cryptococcosis (European blastomycosis)
Cryptospiridosis with diarrhea lasting more than one month.
Cytomegalovirus lesions of any organs (with the exception of organs other than the liver, spleen and lymph nodes) in a patient older than one month.
Infection caused by the herpes simplex virus with ulcerative lesions on the skin (or mucous membranes that persist for more than one month or herpetic bronchitis, pneumonia, or esophagitis of any duration in patients over one month of age).
Kaposi's sarcoma in patients under 60 years of age.
Lymphoma (primary) of the brain in patients under 60 years of age.
Lymphocytic interstitial pneumonia or pulmonary lymphoid hyperplasia (LI/LLH complex) in a child under 13 years of age.
Disseminated infection caused by bacteria of the group with lesions of various organs (with the exception of or in addition to the lungs, skin, cervical or hilar lymph nodes).
Pneumocystis pneumonia.
Progressive multifocal leukoencephalopathy.
Toxoplasmosis of the central nervous system in people older than one month.
The diagnosis of AIDS can also be made with a questionable immunoblot based on the presence of AIDS marker diseases that are reliably confirmed only in cases where the patient has no other reasons for immunodeficiency:
Systemic corticosteroid therapy in large doses or for a long time, as well as treatment with other immunosuppressants or cytostatics three months or less before the onset of AIDS-marker disease.
Any of the following diseases detected within 3 months or less after diagnosis of AIDS marker infection, Hodgkin's disease, non-Hodgkin's lymphoma (except primary brain lymphoma), lymphocytic leukemia, multiple myeloma, other malignant tumors of lymphoreticular or histiocytic tissue, antiimmunoblastic lymphadenopathy.
3. Congenital or acquired immunodeficiency, not similar to HIV infection (for example, accompanied by hypogammaglobulinemia).
With a reliably laboratory confirmed HIV infection, a number of other infections and tumors are included in the list of AIDS indicator diseases:
1) Bacterial infections, combination or recurrent in children under 13 years of age (more than two cases over 2 years of observation) septicemia, pneumonia, meningitis, bone or joint lesions, abscesses caused by Haemophilus influenzae, streptococci.
2) Disseminated coccidioidomycosis (extrapulmonary localization).
3) HIV encephalopathy (“HIV dementia”, “AIDS dementia”).
4) Disseminated hispoplasmosis with extrapulmonary localization.
5) Isosporosis with diarrhea that persists for more than 1 month.
6) Kaposi's sarcoma in people of any age.
7) Brain lymphoma (primary) in people of any age.
8) Other B-cell lymphomas (except for Hodgkin's disease) or lymphomas of unknown immunophonotype:
a) small cell lymphomas (such as Burkitt’s lymphoma, etc.)
b) immunoblastic sarcomas (immunoblastic, large cell, diffuse histiocytic, diffuse undifferentiated lymphomas).
9) Disseminated mycobacteriosis (not tuberculosis) with damage in addition to the lungs, skin of the cervical or hilar lymph nodes.
10) Extrapulmonary tuberculosis (affecting an organ other than the lungs).
11) Recurrent Salmonella septicemia, not caused by Salmonella “Tiffy”
12) HIV - dystrophy.
The rapidly growing number of scientific facts in
virological, immunological and molecular biological fields about the nature of HIV infection in different groups of patients allows
formulate three main questions, the answers to which would significantly advance our understanding of HIV pathogenesis:
1. What factors successfully control the initial acute viremia and suppress HIV replication in the germinal centers of the lymph nodes?
2. What factors cause disturbances in the labile balance between viral replication and control of it by the immune system?
3. What distinguishes patients with long-term incubation period from the majority of HIV-infected people who develop AIDS within a few years?
A distinctive feature of the human immunodeficiency virus is the large variability of different variants of the virus that occurs during infection. It is caused by the key enzyme of HIV replication, reverse transcriptase, which makes errors a million times more often than during the replication of the viral genome than cellular enzymes during the transcription of the cellular genome (one error per thousand base pairs, therefore, ten errors per viral genome).
Since the immune system reacts spontaneously to the predominant viral population and, moreover, with some time lag, newly emerging variants of the virus can multiply in certain cells unhindered for some time. During the course of the disease, new variants of the virus appear, which arise under the selective influence of the patient’s immune system. These virus variants are distinguished by a variety of biological properties. According to the latest classification, corresponding to the current level of knowledge about the virus, variants of the virus are divided into those that reproduce quickly and in high titers in cell cultures (R/H) and those that reproduce only slowly and in small quantities (S/L).
Another criterion is the cytopathogenicity of different variants of the virus, which manifests itself in some cases in the appearance of giant cells, and in others in the fusion of infected cells with uninfected ones to form a functionally incompetent syncytium. These virus variants are designated SI. Virus variants that do not exhibit cytopathogenicity are designated NSI. Research in recent years confirms that virulent and aggressive variants (R/H/SI) arise from less aggressive ones only during the process of HIV infection, caused by the selective influence of the immune system. The emergence of these highly pathogenic variants correlates with the explosive replication of HIV in lymphatic tissues and in the blood with worsening of the clinical picture of the disease.
It is possible to reliably prove the presence of HIV infection and AIDS only by identifying the pathogen itself in the patient’s body. However, this is quite difficult to do. A more common method for diagnosing AIDS is based on the detection of specific antiviral antibodies using various immunological reactions (enzyme immunoassay, fluorescent antibody method, latex agglutination reaction, immunoblotting).
TESTS FOR ANTIBODIES TO HIV (antiHIV-AT).
Over the past three years, HIV antibody tests have greatly changed our understanding of the epidemiology of the virus. Antibodies to HIV appear from three weeks to three months after infection with the virus, and in the future they can almost always be detected, even if the virus does suppress to some extent the function of lymphocytes and the production of antibodies. However, the titer of detectable neutralizing antibodies is low, and the effect is insignificant - they do not noticeably stop the development of infection and disease.
For diagnostic purposes, HIV can be isolated in large quantities from cell lines, purified, and used as an antigen in serological tests. There are several types of anti-HIV tests. Most tests use an antigen-enzyme conjugate, and the signal is a color reaction between a specifically bound enzyme and its substrate. Other tests use radioisotopes, binding of antigen-fluorescein conjugate, or agglutination of virus-coated latex or gelatin particles.
Since anti-HIV tests became commercially available in 1985, they have found widespread use in diagnostic and blood transfusion laboratories. The accuracy of tests - both their sensitivity and specificity - is steadily increasing: cases of false positive and negative responses are becoming less common.
In addition to tests that detect HIV antibodies “in total,” there are more thin tests to identify certain components of the immune response. The response to individual HIV proteins has been studied in detail using immunoblotting and radioimmunoprecipitation methods. Along with this, it is possible to determine individual classes of immunoglobulins in blood and other fluids. Of particular interest are anti-HIV immunoglobulins of class M (IgM), since at the beginning of infection they appear somewhat earlier than IgG antibodies. IgM antibodies are thus formed first in this case.
For mass examinations for anti-HIV antibodies in non-optimal laboratory conditions, simplified test versions are being developed. They are also convenient when the result needs to be obtained urgently, for example, before transplantation. The possibility of using saliva as a diagnostic material is also being considered.
In addition to antibodies, the serum contains viral antigens, in particular, the main protein of the virion core (p24). It can be detected while it is still in excess of antibodies against it, usually at the very beginning of infection. HIV antigen tests are currently being considered for use as an adjunct to antibody tests. They help in diagnosing the early phase of infection, as well as in recognizing infection in children. In later stages, the presence of HIV antigen in the serum indicates immune exhaustion and may serve as an indication for antiviral therapy, the progress of which is then monitored using repeated antigen tests.
Viremia, indicated by the ability to isolate HIV from lymphocytes, can be detected against the background of high titers of anti-p24 and antibodies to other viral proteins. However, virus isolation is a time-consuming procedure, and for successful laboratory diagnosis of HIV in people with little or no antibodies, it is more important to obtain regular follow-up samples. Observations of the development of infection from the moment of infection show that both the titer and the set of antibodies to HIV usually increase. Individuals infected several months ago or earlier almost always exhibit a strong antiviral response. Thus, consistently poor responses to anti-HIV antibodies should be taken with a grain of salt.
In the future, anti-HIV tests are likely to become faster and more practical. Most likely, they will use synthetic antigens and other innovations. Newer anti-HIV test kits can also detect antibodies to related retroviruses such as HIV-2. Perhaps there will also be kits for testing components of the virus - its antigens or genome, as well as kits that can be used independently.
VACCINE DEVELOPMENT OPPORTUNITIES.
Creating a vaccine against AIDS is a complex, multifaceted problem. Such a vaccine must first meet the following requirements:
a) cause neutralization of HIV before it penetrates into the structures of the central nervous system (central nervous system), where the availability of the virus for immunocompetent cells is minimal;
b) ensure recognition by the immune system of all antigenic variants of HIV;
c) guarantee the protection of all vaccinated people, regardless of age and gender, as well as the amount of HIV present in the body;
d) eliminate the risk that the vaccine itself may cause the development of AIDS.
In principle, it is possible to create the following types of vaccines: killed subunit and synthetic. Experiments with inactivated HIV strains as a vaccine are currently being carried out in the J. Salk laboratory (USA). However, due to some risk of developing AIDS during the vaccination process, the scope of application of this biological product is significantly limited. Such a vaccine can only be used to stimulate an immune response in people already infected with HIV (so-called post-exposure prophylaxis). So far, there is no specific data on the clinical results of vaccination carried out by J. Salk.
Immunization against a pathogen that damages an important component of the immune system poses particular challenges. In addition, it turned out that HIV is an extremely variable virus, and the recently isolated HIV-2 is strikingly different from all HIV-1 isolates. Until now, all attempts at immunization against the virus have used purified or cloned envelope glycoprotein. In experimental animals, it does induce the formation of neutralizing antibodies to the virus, but, unfortunately, only to the strain that was used for immunization (type-specific immunity).
Finally, AIDS-related tumors (Kaposi's sarcoma, lymphomas, melanomas, etc.) are usually very malignant, almost resistant to even modern therapy, and very quickly lead patients to a tragic ending.
2) Is it possible to become infected with AIDS in public places? Visiting public places with large crowds of people, among whom may be people with AIDS or infected with the immunodeficiency virus, does not pose any danger in terms of the spread of this infection. It is impossible to become infected with AIDS in a crowd of thousands at a demonstration or rally, when visiting a theater or cinema, while reading a library book or talking on an office telephone.
Without any fear, you can use any type of public transport (metro, bus, tram, etc., including even during peak hours), swim in the pool and exercise in the gym, visit public toilets, get a haircut at a hairdresser and get a manicure. . Without worrying about AIDS, you can occupy a hotel room, even if a sick person previously lived in it, and live in a camp site, half of the inhabitants of which sneeze or cough. In such living conditions, you can become infected with the flu or an acute respiratory disease, in extreme cases, measles or mumps (if you did not have these infections in childhood and for some reason were not vaccinated), but not AIDS.
3) Is it possible to get AIDS from kissing? This question is very complex and still does not seem to have a clear answer. Of course, there is always a small amount of viral particles in the saliva of an infected person, and with so-called “wet” (“sexy”) kisses they can enter the body of a healthy person. Therefore, theoretically, you can become infected with the immunodeficiency virus through kissing, especially if you kiss often, for a long time and with everyone. And if at the same time you enter into intimate contact with a casual partner, then you can’t avoid AIDS. But with “dry” kisses, comradely ones - on the cheek, gentlemanly ones - on the fingers or hand of a lady, parents, etc. HIV transmission is virtually eliminated. And for girl brides or boy grooms who are going to enter into a legal marriage and then become faithful spouses, there is no reason to worry about AIDS during mutual kisses both before and after the wedding.
4) Does a condom protect against AIDS? The use of condoms reduces the likelihood of immunodeficiency infection. For example, during a survey of 526 prostitutes in the United States, antibodies to the AIDS pathogen were found in 11% of these women. At the same time, all 22 prostitutes, whose clients always used condoms, had negative serological tests for HIV. However, it should be remembered that mechanical contraceptives, even when used correctly, do not provide a 100% guarantee of preventing AIDS (the probability of infection through constant contact with an infected sexual partner throughout the year will be about 10-15%). It should be emphasized once again in conclusion that the most effective preventive measure against AIDS is still the prevention of casual sexual intercourse.
5) How can AIDS not be transmitted? The causative agents of AIDS are contained in large quantities in the blood, other biological fluids and various secretions of the patient. However, for surrounding healthy people in everyday conditions, a person infected with HIV infection or suffering from AIDS poses virtually no danger as a source of infection. This is explained by many reasons (a rapid decrease in the number of viable viral particles; their inability to penetrate the human body through intact skin or mucous membranes; low probability of direct and prolonged contact of a healthy person with infectious material located in the external environment, etc.).
The results of long-term observations of tens of thousands of AIDS patients have clearly proven that AIDS pathogens are not transmitted through handshakes or hugs, through dishes or household items, bed or underwear, coins or paper banknotes. Even the slightest possibility of contracting AIDS through food, drinking water, fruit and vegetable juices, indoor air or atmospheric air is excluded. Not a single case of AIDS has been registered in which infection occurred through toys or school and writing materials, although children have household contact with each other more frequently and directly than adults. So the conclusion can be drawn unequivocally: AIDS pathogens are not transmitted from infected or sick people to healthy people through everyday contact!
6) What is the forecast for the development of the AIDS epidemic? The World Health Organization estimates that the total number of AIDS patients will exceed 2 million at the end of 1997, and will reach several million by the year 2000. Probably about 500 thousand newborns will be infected with AIDS and most of them will die in the first 3-5 years. Forecasts showed that in 1989 the number of AIDS patients in Europe should have exceeded 20 thousand (the forecast was justified), and in 1990 it should have reached 100 thousand. In North America and most European countries, the number of people infected with the AIDS virus will continuously increase in risk groups, in particular among drug addicts. However, a significant increase in incidence is expected among ordinary people who do not belong to risk groups. This is due to the widespread heterosexual transmission of HIV.
7) Are there any achievements in the fight against AIDS? Without a doubt. First of all, this is the creation, under the auspices of WHO, of the Global Program on AIDS - a special group of scientists to organize the fight against AIDS and HIV infection. This group includes about two hundred highly qualified specialists.
An AIDS surveillance system has been developed and is successfully functioning, in which 177 countries of the world participate (as of January 1, 1989, about 133 thousand cases of AIDS were registered in 143 countries). An expert assessment of the incidence of HIV infection in the world was carried out, based on scientific epidemiological data (Africa - 2.5 million, America - 2 million, Europe - 500 thousand, Asia and Oceania - 100 thousand). Adequate experimental models of AIDS and HIV infection have been developed in various laboratory animals (mice, rabbits, etc.).
In recent years, new diagnostic test systems have been created that make it possible to detect antibodies to HIV within 1-5 minutes and are not inferior in quality (primarily in sensitivity and specificity) to a standard enzyme-linked immunosorbent assay. Four vaccines created using genetic engineering methods are already undergoing the first phase of clinical trials on humans. More than 50 new chemotherapy drugs with high activity against HIV are undergoing clinical trials.
"10 Commandments about AIDS"
1) AIDS is a completely new disease that is widespread throughout the world.
2) The paths and spread of the AIDS virus are already well known.
3) To know the ways in which the AIDS pathogen spreads means to know how to prevent it.
4) Sexual transmission of the AIDS virus can be prevented.
5) There are various reliable ways to prevent the transmission of infection through blood.
6) It is very important to know how the AIDS pathogen does not spread.
7) You should not be afraid of communicating in everyday life with people infected with the AIDS virus.
8) Since there are still no vaccines against AIDS and absolutely reliable drugs, truthful information and health education play a vital role in preventing infection.
9) Currently, all countries of the world are rising to fight the global threat of AIDS.
10) Together we can stop the spread of AIDS!
RUSSIAN scientists have invented an AIDS vaccine.
If the clinical trials are successful, in 5 years anyone will be able to get vaccinated and breathe a sigh of relief, without fear that HIV infection will take him to the grave.
WHY can’t we take advantage of the discovery now? The vaccine, which the AIDS Center of the Institute of Immunology of the Ministry of Health of the Russian Federation worked on from 1997 to 2002, has passed the experimental stage of testing. Mice and rabbits suffered for humanity. Now we need to make sure that the vaccine is safe and effective for people too. Clinical trials will be conducted on healthy people at risk. They will mainly recruit drug addicts, because in Russia every ninth person becomes infected through a dirty syringe. And, despite the fact that anyone has a chance of catching the virus, it is much higher for drug addicts. The contingent is undisciplined, unreliable, someone may die from an overdose before the tests are completed, but scientists hope for success.
Despite the poverty of the state, it was precisely this state, thanks to the State Duma Committee on Science and Education, that found the opportunity to finance the program “New Generation Vaccines and Medical Diagnostic Systems of the Future” under the auspices of the Ministry of Industry and Science. It is unknown whether the funds allocated from the budget will be enough for the upcoming clinical trials, the most complex and expensive ones. The Americans promised to support our scientists financially this summer.
Immune stimulant
“The VACCINE was not created exactly according to the principle on which all existing vaccines operate - from influenza, measles, smallpox, etc.,” says the head of the AIDS Center of the Institute of Immunology of the Ministry of Health of the Russian Federation, Doctor of Medical Sciences, Professor Igor Sidorovich. “The problem is , that if a person recovers from these diseases, he acquires immunity to them. But there are still no people who have recovered from AIDS, so we do not know what the natural protection against the disease is, and we cannot use a weakened AIDS virus in the vaccine. The task of the vaccine is to introduce artificial antigens to a person, copying the most important parts of the AIDS virus, and thereby prepare the body for a possible encounter with infection: force it to produce special defenses (antibodies that neutralize the virus floating in the blood, and killer cells that will kill already infected cells) ", that is, if the virus enters the body, "specially trained" immune forces will be waiting for it there and will destroy it. We hope that the clinical trials will be successful, but in parallel we are developing a series of other, more advanced vaccines."
To launch mass production of a vaccine, you will not need to build new factories or purchase super expensive equipment. Biotechnology is a very expensive industry at the research and development stage. But once the vaccine is received and tested, it will take 20 large, very clean rooms and 20 well-educated specialists to provide it to the entire country.
Chosen Among Us
ANOTHER chance to protect yourself from the plague of the twentieth century was provided by nature itself - this is a paired mutation of the CCR5 genes. Scientists have noticed that some people - sexual partners of HIV-infected people - do not become infected. They were examined and found that they had something in common that protected them from the virus - the mutated CCR5 gene. “The majority of people with this gene mutation live in Scandinavia,” says Sergei Apryatin from the Laboratory of Biotechnology and AIDS at the Institute of Immunology. “It is extremely rare in Africa and Australia. Europeans are the layer between north and south where people with this mutation are found quite often "Unfortunately, the protection factor only works during sexual transmission, because upon contact with blood there are no barriers to the virus."
You can find out if you are one of the lucky ones with a blood test. There are many couples in Russia where one of the partners is infected, and the other is protected from the virus by a pairwise mutation of the CCR5 genes. With their help, scientists are studying the possibilities of natural defense against the deadly virus and hope to defeat it on the other side. Scientists do not yet know the nature of other protective mechanisms, but they exist. For example, in Africa, where HIV infection has become an epidemic, some prostitutes who are constantly in contact with infected men are themselves resistant to infection, although they do not carry the CCR5 gene mutation. Scientists are now trying to understand what exactly protects them.
All these developments cost money. Losses from AIDS can be compared with the losses of humanity in World War II - 60 million infected, 25 million have already died. Huge amounts of money were invested in winning the war. To overcome AIDS, you need to invest no less.
In the relatively short time for the history of medicine that has passed since June 1981, when the socialists of the Center for Disease Control (Atlanta, USA) paid special attention to information about 5 patients with Pneumocystis pneumonia and candidiasis, an unprecedentedly large amount of scientific research has been carried out on the problem HIV infection, effective laboratory diagnostic methods have been proposed. However, to date, diagnosing HIV infection has often been difficult.
Considering that AIDS is considered a disease with 100% mortality, as well as the wary public orientation towards HIV-infected people, establishing such a serious diagnosis imposes special responsibility on doctors for the psycho-emotional state, social adaptation, and sometimes even for the life of the patient (infected).
The main task of laboratory diagnosis of HIV infection is to identify the primary infection as early as possible in order to:
- protection of blood recipients, organs and tissues;
- prescribing and carrying out antiviral therapy;
- carrying out anti-epidemic measures.
Ignorance of the etiology, pathogenesis, and clinical course of the disease makes it difficult to interpret the results of clinical and laboratory studies. The problem of laboratory diagnosis of HIV infection is aggravated by the imperfection of diagnostic test systems, caused, on the one hand, by technological difficulties, on the other, by the high genetic variability of the virus and the similarity of the antigenic composition of HIV and some structures of the human body.
ETIOLOGY
The source of HIV infection is humans. Viral particles are found in many biological fluids of infected people - in blood, semen, cerebrospinal fluid, breast milk, vaginal and cervical secretions. This leads to several routes of transmission of HIV infection. HIV can be transmitted through sexual contact, transfusion of blood and blood products, use of contaminated medical instruments, from mother to child and from child to mother during breastfeeding, as well as from mother to child during pregnancy and childbirth.
HIV belongs to the retrovirus family and the lentivirus subfamily (Fig. 9.1). Members of the retrovirus family are characterized by their genomic RNA content and the enzyme reverse transcriptase (revertase). In order for the retrovirus genome to connect with the cell genome, DNA is first synthesized from the viral RNA template using reverse transcriptase. The proviral DNA is then integrated into the genome of the host cell.
History of the discovery of HIV
HIV was discovered almost simultaneously in 1983, independently of each other, by two researchers - R. Gallo (National Cancer Institute, USA) and L. Montagnier (Institut Pasteur, France).
R. Gallo discovered the first human retrovirus in 1980. The virus affected T-cells of the blood, causing leukemia, and received the corresponding name - human T-cell leukemia virus, Human T-cell Leukemia Virus (HTLV). Next, the retrovirus HTLV-II, which causes chronic hairy cell T-leukemia, was isolated in R. Gallo's laboratory.
The new infectious disease AIDS, unknown until 1981, was accompanied by a depletion of the pool of T-lymphocytes, which prompted R. Gallo to think about the connection of this disease with an unknown T-lymphotropic virus. The studies that resulted in the isolation of HTLV-III confirmed the scientist’s hypothetical assumptions.
In the laboratory of L. Montagnier, a new virus was isolated from a patient with lymphadenopathy syndrome and named lymphadenopathy-associated virus (Lymphadenopathy associated Virus (LAV)). After it was established that HTLV-III and LAV were the same virus, a single term was adopted - the human immunodeficiency virus, HIV (Human Immunodeficiency Virus, HIV). However, the names of commercial test systems for determining antibodies to HIV sometimes contain the same designations of the virus.

HIV includes two main structures - the envelope and the nucleoid/nucleocapsid (core part) (Fig. 9.2). The viral envelope is a fragment of the membrane (outer or endoplasmic reticulum) of the host cell in which the virion was assembled. The lipid layer carries the glycoprotein gp160* (* The Latin letters gp denote glpcoprotein, and the number corresponds to the molecular weight of the protein in kilodaltons, kDa), consisting of an extramembrane (outer) part, designated gp120, and a transmembrane part, gp41. The transmembrane protein GP41, located directly in the virus envelope, is connected by disulfide bonds to several (3 to 6) GP120 molecules. A certain amount of glycoprotein gp120 is randomly separated from the virion and enters the blood and body tissues in the form of a soluble substance.
Inside, under the shell, there is a matrix frame consisting of the protein p17/18** (** The Latin letter p stands for protein. The "/" sign indicates the molecular weight of the protein according to various literature sources. Below in the text the most frequently used in practice will be given values).
The HIV nucleoid has the shape of a rod-shaped or conical capsule, characteristic of retroviruses. The nucleoid wall consists of the p24/25 protein. The core of the virion contains two single-stranded RNA molecules, with which proteins p7 and p9 are associated, as well as a complex of enzymes: reverse transcriptase (revertase), integrase (endonuclease), RNaseH and protease.
L. Montagnier's collaborators in 1986 managed to isolate a variant of the human immunodeficiency virus from two Africans with an AIDS-like disease. The virus was not recognized by HIV antibodies, so it was designated HIV-2. Within two years, the disease caused by HIV-2 was identified on other continents. It is characterized by a longer asymptomatic period compared to HIV-1 infection.
The structure of HIV-2 is identical to the structure of HIV-1. However, most of the structural proteins differ in molecular weight and antigenic characteristics. For example, the surface epimembrane and transmembrane glycoproteins have a different molecular weight than gp120 and gp41, and are designated gp105/125* (* In the works of some authors, the epimembrane glycoprotein gp105 is designated as gp125) and gp36, respectively. gp105 has the same pronounced affinity for receptor proteins of target cells as gp120. The HIV-2 nucleocapspd consists of the p26 protein, and the matrix framework consists of the p16 protein.
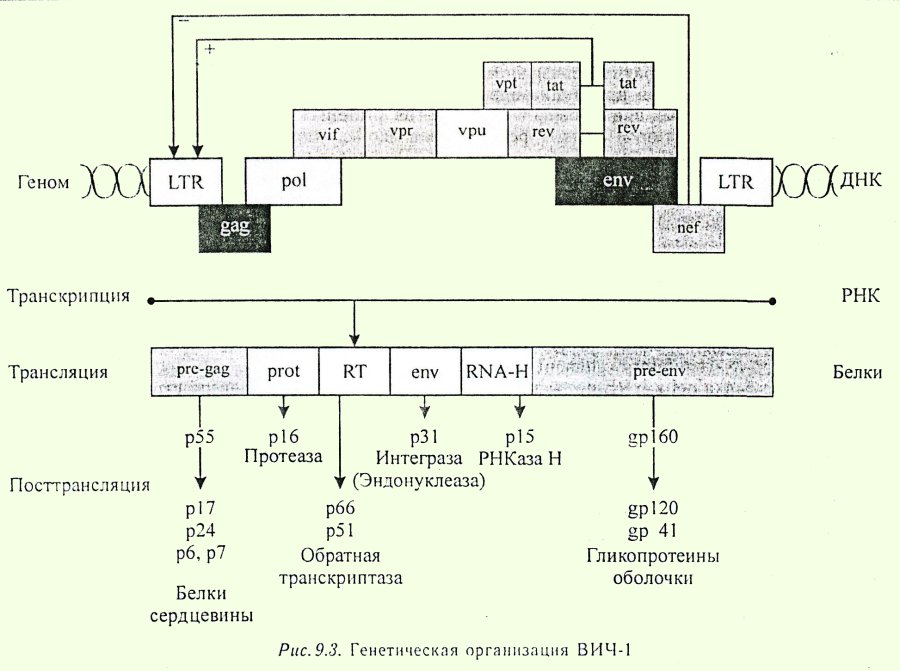
HIV genome
The HIV-1 genome is represented by three large structural and seven small regulatory genes (Fig. 9.3). Genes on both sides of the polynucleotide chain are bounded by so-called long terminal repeats (LTR). Long terminal repeats are sections of DNA that contain a number of important regulatory fragments. These include binding sites for factors influencing the transcription process: the area (site) from which transcription begins - messenger RNA from provirus DNA, and nucleotide sequences necessary for initiation (promoter), amplification (enhancer) and inhibition (negative regulation element) transcriptions. Thus, the LTR performs key regulatory functions by mediating and controlling the initiation and rate of viral replication.
Structural genes encode proteins that are directly included in the structure of the virion or are enzymes. These include genes designated env, gag and pol.
- Gene env (from the English envelope - shell) [show]
.
encodes the translation of a protein with a molecular weight of 160 kDa, which is the precursor of the viral envelope glycoproteins gp41 and gp120.
- The gag gene (from the English group specific antigens - group-specific antigens) [show]
.
encodes the synthesis of the p55 protein, which is the precursor of the four internal proteins of the virus - p24 (nucleocapsid), p17 (matrix framework), p7 and p6. The p7 protein is associated with the genomic RNA of the virus and is necessary during the assembly of the virion to enclose the RNA in the nucleocapsid.
The p6 protein ensures the release of daughter virnons from the host cell.
- Gene pol (from English polymerase - polymerase) [show]
.
encodes the synthesis of protease (p52/53), which cleaves the p55 precursor protein (gag), and three other enzymes - reverse transcriptase (revertase) (p64/66/68). RNase H (p15), which separates the RNA molecule from the complex of complementary RNA+DNA chains formed during reverse transcription, and integrase (p31/32), which ensures the integration of proviral DNA into the host cell genome.
All 4 enzymes, as mentioned above, are concentrated in the nucleocapsid of the virion.
Below is a summary of HIV-1 regulatory genes, the products of which regulate or provide processes associated with the replication cycle of the virus in the cell.
- Gene tat (from the English transactivator of transcription - transcription transactivator) [show]
.
It consists of two spatially separated sections and is responsible for activating the transcription of provirus genes. Tat is called a transactivator because it affects genes not located in its immediate vicinity. The tat gene encodes the synthesis of the so-called transactivating factor - a protein with a molecular weight of about 14 kDa, found in the nucleus and cytoplasm of HIV-affected cells.
This protein is necessary for the full biosynthesis of viral RNA and is capable of increasing the synthesis of viral proteins by more than 1000 times at the stages of both transcription and translation. Tat acts on both proviral and human genes, being a growth factor for Kaposi's sarcoma cells.
An increase in the synthesis of viral proteins resulting from the action of tat gene products stimulates the production of the transactivating factor itself, which, in turn, through a positive feedback mechanism leads to even more intense production of viral proteins and the assembly of new virions.
- Rev gene (from the English regulator of virus - virus regulator) [show]
.
encodes the synthesis of a protein with a molecular weight of about 19 kDa, which is localized in the nuclei of infected cells.
The presence of the protein accelerates the process of transport of viral messenger RNA from the nucleus to the cytoplasm.
- The nef gene (from the English negative regulatory factor - negative regulatory factor) [show]
.
encodes the synthesis of a protein with a molecular weight of 24-25/27 kDa, which has an affinity for the long terminal repeat region - the negative regulatory element (NRE). The interaction of the nef protein and NRE leads to suppression of mRNA transcription and, as a consequence, to a decrease in the synthesis of viral proteins.
- The function of a protein with a molecular weight of 23 kDa - the product of the vif gene (from the English viral infectivity factor - factor of the infectivity of the virus) - has not been definitively established. It is believed that the named protein increases the infectious ability of newly formed virions.
- Regulatory gene vpr (from the English virus protein K - viral protein K) [show]
.
encodes the synthesis of a protein with a molecular weight of 15 kDa. This protein provides the activating function of the long terminal repeat (LTR), is part of daughter virions and activates transcription from genomic RNA after virus entry into the cell.
- The significance of the regulatory gene vpl (from the English virus protein T - viral protein T) has not been established.
- Regulatory gene vpu (from the English virus protein U - viral protein U) [show]
.
encodes the synthesis of a protein with a molecular weight of 16 kDa. This protein plays a role in the assembly of virions and their separation from the host cell.
The existence of gene mechanisms for both activation (tat, rev genes) and inhibition (nef gene) of the HIV replication process provides a state of functional equilibrium in which the provirus can be in an inactive form.

The HIV-2 genome is similar in structure to the HIV-1 genome (Fig. 9.4). The difference between the genomes is that HIV-2 does not have the vpu regulatory gene, but there is a vpx regulatory gene, which is absent in HIV-1, located in the provirus genome similar to the vpu gene. The homology of the nucleotide sequences of HIV type 1 and type 2 genes is approximately 50%.
HIV variability
HIV variability is associated with inaccurate operation of reverse transcriptase during proviral DNA synthesis. Based on differences in the nucleotide sequences of the env gene and, accordingly, in the amino acid sequences of gp120, HIV variants are divided into three groups: M (major), O (outline) and N (non M and O).
The region of the gp120 molecule that forms the loop-shaped domain (the so-called V3 loop of 35 amino acids) is characterized by the greatest variability. 80-95% of antiviral antibodies are specific to this site.
The main group M (from the English major - main) dominates the world today. It, in turn, is divided into subtypes, designated by letters of the Latin alphabet from A to H. HIV variants of this group are found in all countries. The geography of distribution of subtnps is as follows. In Africa - the cradle of HIV - all subtypes have been identified. In Europe and North America, subtype B prevails, in Southeast Asia - subtype E, in India - subtype C. In general, the following frequency of isolation of HIV subtypes in infected individuals is observed in the world (Fig. 9.5).

In all regions of the world, so-called recombinant subtypes are found, containing part of the genes of one subtype and part of another. So in Russia, the main subtype of HIV is A, but A+B recombinants are found.
The group of strains O (from the English outline) has significant genetic differences from the representatives of the main group. Cases of infection with HIV-0 strains occur in West Africa, their number is still small. At the same time, a number of leading manufacturers of enzyme-linked immunosorbent test systems for determining antibodies to HIV include HIV-O antigens in the kits, since it is likely that this subtype of the virus will quickly spread outside Africa.
HIV-2 also has several subtypes.
Determination of HIV subtypes is carried out using molecular biology methods - polymerase chain reaction (PCR) and the bDNA method, based on the use of branched DNA probes (branch DNA). The bDNA method allows quantitative determination of HIV RNA and HIV provirus DNA, including all 5 main subtypes.
Commercial kits designed to determine HIV RNA by PCR are designed to detect all types of HIV except D.
Genetic variability is manifested in variability not only in the antigenic, but also in the biological properties of virus isolates.
| Page 1 | total pages: 8 |
LITERATURE [show] .
- Federal Law of the Russian Federation "On preventing the spread of Russian Federation disease caused by the human immunodeficiency virus" dated March 30, 1995.
- Zmushko E.I., Belozerov E.S. HIV infection / Guide for doctors. - St. Petersburg: Peter, 2000. - 320 p.
- Isakov V. A., Aspel Yu. V., Bogoyavlensky G. V. et al. Experience of using cycloferon in the treatment of HIV infection and AIDS / Guide for doctors. - St. Petersburg, 1997. - 60 p.
- Kozhemyakin L. A., Bondarenko I. G., Tyaptin A. A. Acquired immunodeficiency syndrome / Manual for doctors. - L.: Knowledge, 1990. - 112 p.
- Lobzin Yu. V., Kazantsev A. P. Guide to infectious diseases. - St. Petersburg, 1996. - 712 p.
- Lysenko A. Ya., Turyanov M. X., Lavdovskaya M. V., Podolsky V.M. HIV infection and AIDS-associated diseases / Monograph. - M.: Rarog LLP, 1996, - 624 p.
- Novokhatsky L. S., Khlyabich G. N. Theory and practice of laboratory diagnosis of acquired immunodeficiency syndrome (AIDS). - M.: VINITI, 1992, - 221 p.
- Pokrovsky V.I., Pokrovsky V.V. AIDS: acquired immunodeficiency syndrome. - M.: Medicine, 1988. - 43 p.
- Pokrovsky V.I. HIV infection or AIDS // Therapist, architect. - 1989. - T. 61, No. 11. - P. 3-6.
- Pokrovsky V.V. HIV infection: clinic, diagnosis / Ed. ed. V.V. Pokrovsky. - M.: GEOTAR MEDICINE, 2000. - 496 p.
- Rakhmanova A. G. HIV infection (clinic and treatment). - St. Petersburg: "SSZ", 2000. - 367 p.
- Recommendations for the use of antiretroviral drugs in adults and adolescents infected with the human immunodeficiency virus // Consilium Medicum appendix. January 2000, - 22 p.
- Smolskaya T. T., Leninskaya P. P., Shilova E. A. Serological diagnosis of HIV infection / Methodological manual for doctors. - St. Petersburg, 1992. - 80 p.
- Smolskal T. T. The second decade of life in conditions of SSDA: lessons and problems / Actual speech. - St. Petersburg, 1997. - 56 p.
- Khaitov R.M., Ignatieva G.A. AIDS. - M., 1992. - 352 p.
- Connor S. Research shows how HIV exhausts the body // Brit. Mod. J.- 1995.- Vol.310.- P. 6973-7145.
- Burcham J., Marmor M., Dubin N. et al. CD4 is the best predictor of development of AIDS in a cohort of HIV-infected homosexual men // J. AIDS. - 1991. - jN"9. - P.365.
- Furlini G., Vignoli M., Re M. C., Gibellini D., Ramazzotti E., Zauli G.. La Placa M. Human immunodeficiency virus type I interaction with the membrane of CD4+ cells induces the synthesis and nuclear translocation of 70K heat shock protein //J.Gen. Virol.- 1994.- Vol.75, pt 1.- P. 193-199.
- Gallo R. C. Mechanism of disease induction by HIV // J.AIDS.- 1990.- N3.- P. 380-389.
- Gottlieb M. S., Schroff R., Schanker H. et al. Pneumocystis carinii pneumonia and mucosal candidiasis in previously homosexual mon // Now England J. Med. - 1981. - Vol. 305. - P. 1425-1430.
- Harper M. E., Marselle L. M., Gallo R. C., Wong-Staal F. Detection of lymphocytes expressing human T-lymphotropic virus type III in lymph nodes and peripheral blood from infected individuals by in situ hybridization // Proc. Natl. Acad. Sci. U.S.A. - 1986. - Vol. 83. - N 2. - P. 772-776.
- Hess G. Clinical and diagnostic aspects of HIV infection.- Mannheim: Boehringer Mannheim GmbH, 1992.- 37 p.
- Hu D. J., Dondero T. J., Ryefield M. A. et al. The emerging genetic diversity of HIV // JAMA.- 1996. - N 1.- P. 210-216.
- Lambin P., Desjobert H., Debbia M. et al. Serum neopterin and beta-2-microglobulin in anti-HIV positive blood donors // Lancet.- 1986.- Vol. 8517. - P. 1216.
- Maldonado I. A., Retru A. Diagnosis of pediatric HIV disease // The AIDS knowledge base, Fd. Cohen P.T.; Sande M. A. Voiberding. 1994.- P. 8.2.1-8.2.10.
- McDougal J.S., Kennedy M.S., Sligh J.M. et al. Binding of the HTLV-III/LAV to T4+ T cells by a complex of the 110K molecule and the T4 molecule // Science.- 1985.- Vol.23.- P. 382-385.
- Montagnier L., Gougeon M. L., Olivier R. et al. Factors and mechanisms of AIDS pathogenesis // Science challenging AIDS. Basel: Karger, 1992.- P. 51-70.
- Paterlini P., Lallemant-Le C., Lallemant M. et al. Polymerase chain reaction for studies of mother to child transmission of HIV-I in Africa // J.Med. Virol. - 1990.- Vol.30, N 10.- P. 53-57.
- Polis M. A., Masur H. Predicting the progression to AIDS // Amor. J. Med. - 1990.- Vol.89, N 6.- P. 701-705.
- Roddy M.M., Grieco M.H. Elevated soluble IL-2 receptor levels in serum of HIV infected populations // AIDS Res. Hum. Retrovir. - 1988.- Vol.4, N 2. - P. 115-120.
- Van dor Groen. G., Van Kerckhoven I. et al. A simplified and less expensive, in comparison with the traditional, method of confirming HIV infection // Bulletin. WHO.- 1991.- T. 69, No. 6.- P. 81-86.
Source: Medical laboratory diagnostics, programs and algorithms. Ed. prof. Karpishchenko A.I., St. Petersburg, Intermedica, 2001
Human immunodeficiency virus is a retrovirus, genus lentivirus. Externally, it has the shape of a sphere, the diameter of which is from 120 to 150 nm. The outer shell, through which HIV binds to cells of the immune system, contains several proteins - glycoproteins (gp41-transmembrane and gp120-surface). Surface glycoproteins form peculiar outgrowths on the virus membrane, reminiscent of appearance(in an electron microscope) the “cap” of the mushroom, and gp41 is its “leg”. The basis of the virus - the genome - is represented by single-stranded RNA (two molecules). Each molecule is represented by nine viral genes: structural, regulatory and accessory. They, accordingly, carry information about the structure of the virus, methods of infecting cells, and the reproduction of virions.
 The viral genome is surrounded by matrix and capsid proteins (p17 and p24, respectively), forming a closed cone-shaped structure. HIV has the ability to produce enzymes such as reverse transcriptase, protease and integrase. In addition, the human immunodeficiency virus can change extremely quickly under the influence of mutations in its genome. Most variants of the virus differ from each other very little, but several species have been identified with significant differences: HIV-1 (discovered in 1983), HIV-2 (in 1986), HIV-3 (in 1988) and HIV-4 (first discovered in 1986, but identified as a separate species somewhat later). HIV-1 affects mainly the population of Europe and America, HIV-2 – West Africa, other types of the virus are not so widespread.
The viral genome is surrounded by matrix and capsid proteins (p17 and p24, respectively), forming a closed cone-shaped structure. HIV has the ability to produce enzymes such as reverse transcriptase, protease and integrase. In addition, the human immunodeficiency virus can change extremely quickly under the influence of mutations in its genome. Most variants of the virus differ from each other very little, but several species have been identified with significant differences: HIV-1 (discovered in 1983), HIV-2 (in 1986), HIV-3 (in 1988) and HIV-4 (first discovered in 1986, but identified as a separate species somewhat later). HIV-1 affects mainly the population of Europe and America, HIV-2 – West Africa, other types of the virus are not so widespread.
Interaction of HIV with a cell
 HIV can only interact with cells that carry CD4 receptors on their surface. These cells are mostly macrophages and T-lymphocytes. The surface glycoprotein (g120) on the virus membrane ensures contact with the CD4 receptor of the lymphocyte cell, as a result of which they merge with each other, and the HIV genetic material penetrates into the cytoplasm. The reverse transcriptase of the virus at this moment starts the process of DNA synthesis based on one strand of its own RNA, i.e. directly activates reverse transcription. The enzyme integrase then starts the process of joining the host and newly synthesized viral DNA. In addition, the cell is rebuilt to synthesize viral RNAs instead of its own, as a result of which the cell’s ribosomes, instead of their own proteins and enzymes, begin to produce viral enzymes and its structural proteins in huge quantities. The process of producing virions inside the cell, which is catalyzed by a protease, starts. As soon as their number becomes excessively large, they, having destroyed the cell membrane, enter the outside - into the blood, where they infect new lymphocytes and macrophages.
HIV can only interact with cells that carry CD4 receptors on their surface. These cells are mostly macrophages and T-lymphocytes. The surface glycoprotein (g120) on the virus membrane ensures contact with the CD4 receptor of the lymphocyte cell, as a result of which they merge with each other, and the HIV genetic material penetrates into the cytoplasm. The reverse transcriptase of the virus at this moment starts the process of DNA synthesis based on one strand of its own RNA, i.e. directly activates reverse transcription. The enzyme integrase then starts the process of joining the host and newly synthesized viral DNA. In addition, the cell is rebuilt to synthesize viral RNAs instead of its own, as a result of which the cell’s ribosomes, instead of their own proteins and enzymes, begin to produce viral enzymes and its structural proteins in huge quantities. The process of producing virions inside the cell, which is catalyzed by a protease, starts. As soon as their number becomes excessively large, they, having destroyed the cell membrane, enter the outside - into the blood, where they infect new lymphocytes and macrophages.
Structure and chemical composition
The structure of HIV-1 and HIV-2 is similar to other lentiviruses. The HIV virion is spherical, 100-200 nm in diameter. The outer shell of virions is formed by a double lipid layer, which is borrowed by the virion from the host cell membrane upon completion of the replication cycle and exit from the cell. The virion shell contains a glycoprotein complex of the virus, consisting of two subunits (gp41, gpl20) with a non-covalent bond between them. The transmembrane protein gp41 penetrates the viral envelope, the second protein, gp 120, forms processes (“spikes”) on the surface of the virions. On the inside of the lipid envelope there is a matrix frame formed by the p17/18 protein. The core of the virion is cylindrical or cone-shaped, formed by the capsid protein p24. The core of the virus contains the nucleocapsid protein p7/p9, the viral genome - two single-stranded RNA molecules and three viral enzymes - reverse transcriptase, protease and integrase. The HIV genome contains 104 nucleotides and is represented by 9. Three structural genes gag, pol and env encode components of viral particles : gag gene - internal group-specific proteins of the virion that are part of the core and capsid (p24, p7/9, p17), env gene - type-specific proteins that are part of the outer shell (gp41 and gpl20), pol gene - proteins of viral enzymes The HIV genome also contains six regulatory genes encoding small proteins involved in the system for regulating the activity of structural genes. HIV-1 and HIV-2 have genes tat, rev, nef, vif, vpr. In addition, HIV-1 also has a vpu gene, and HIV-2 has a vpx gene. Within the total length of the genome, the genes partially overlap with neighboring ones; the two tat u rev genes each consist of two segments quite far apart from each other. Tat protein - transcription transactivator, necessary for the biosynthesis of the full-length viral RNA transcript; it increases the transcription rate of both structural and regulatory viral proteins tens of times. The Rev protein ensures the transport of unspliced or singly spliced viral RNA from the nucleus into the cytoplasm, where Gag/Pol or Env proteins are translated from it. In the absence of the rev gene product, structural proteins are not formed at all. The importance of the Nef protein has been evident since its discovery, but its functional purpose continues to be debated. According to recent data, the function of the Nef and Vpu proteins is aimed at reducing the expression of cellular CD4 receptors in the infected cell. Tat, Rev and Nef proteins are not part of the virion, but are the first viral components that are synthesized during the viral replication cycle. A distinctive feature of retroviruses in general, and HIV in particular, is their high variability compared to the range of variability of other viruses. It was in relation to retroviruses that the concept of quasi-species was introduced, since even within the same organism, subsequent generations of the virus differ from the parent ones. The probability of mutation for HIV-1 is estimated to be 10-4-10~5 per replication cycle. B life cycle HIV point mutations can occur at the stage of reverse transcription from genomic RNA to the “minus” DNA strand, at the stage of synthesis of the “plus” DNA strand when a provirus appears, and, finally, during transcription of RNA from provirus DNA. Deletions and insertions are also possible, but the probable frequency of their occurrence is difficult to estimate. The highest variability in nucleotide composition is characteristic of the env gene. The degree of variability varies in different parts of the molecule of the encoded envelope protein. More than 20 functionally significant sequences (sites or epitopes) have been mapped in the gpl20 and gp41 shell proteins. The variable regions of gpl20 V1-V3 are associated with the phenotypic properties of the virus, as well as tropism for chemokine receptors, with the hypervariable region V3 - the immune response and the ability of the virus to “escape” pressure from the immune system. Three different regions of gp 120 are important for recognition of the CD4 receptor and binding to it. When the gpl20 molecule is in a spatial configuration, these regions are brought closer together, forming a cavity corresponding to the CD4 receptor. Systematization of the genetic diversity of HIV-1 based on analysis of the nucleotide sequences of the env and gag genes was carried out according to the position of various strains on a rootless phylogenetic tree. HIV-1 strains circulating in different regions of the world are grouped into two different groups. The majority of known epidemic strains belong to the first large group M (major). Within the M group, at least 10 genetic subtypes are classified, each of which is designated by letters of the English alphabet from A to J. The difference in the nucleotide sequence of the V3 region of the env genes of isolates belonging to the same subtype is 5-15%, while between different subtypes - 16-30%. Differences in the genomes of viruses from one patient in the dynamics of the disease, as a rule, do not exceed 5%, and from different people 0.5 -0.4%. A great contribution to the study of the evolution of HIV-1 is made by the recombinant forms of the virus discovered in recent years, which caused the largest epidemic among the heterosexual population in Thailand (E/A recombinant) and local epidemics among drug addicts in two provinces of China (B/C recombinant) and Kaliningrad region in Russia (A/B recombinant). In addition to group M, in 1994, another small group of highly divergent HIV-1 strains was identified from patients of African origin - group “O” (English Outliner). The differences in the nucleotide sequence of group O viruses as a whole compared to group M are about 35%, and in the env gene - 56%.Pathogenesis and immunity
In general terms, the disease caused by HIV can be characterized as an immunodeficiency state of an infectious nature, resulting from the ability of the virus to parasitize directly in the cells of the immune system. Almost with the same frequency as the immune system, the nervous system is also affected by HIV infection. The pathogenesis of HIV infection is a complex process of many years of interaction between the pathogen and the host body from the moment of primary infection to the last fatal stage of the disease. Human infection occurs when virus-containing materials enter the mucous membranes of the genitals or rectum, directly into the blood, as well as through the infected placenta. Direct “target” cells for HIV are cells that have CD4 receptors on their surface, which are most represented on the membrane of helper T-lymphocytes. Many other cells also have CD4 receptors (monocytes and their tissue forms - macrophages, Langerhans cells, follicular cells of lymph nodes, alveolar macrophages of the lungs, microglial cells, etc.). However, it is known that HIV can also infect cells that do not have CD4 receptors (astrocytes, endothelial and epithelial cells). The latest research into the tropism of the virus to various chemokine receptors will obviously provide additional information about the mechanisms of development of HIV infection. Dendritic cells (especially Langerhans cells when infecting mucous membranes) and monocytes / macrophages are among the first to become infected and, through circulation, deliver the virus into the blood and into the nearest lymphoid organs, presenting the virus to T4 lymphocytes. During parenteral infection, the virus can directly infect T4 lymphocytes. It has been shown that viruses isolated at the initial stages of the disease are mainly macrophagotropic. HIV replicates in macrophages/monocytes with moderate intensity and, leaving the cell, does not have a cytolytic effect on it. These cells are a chronic reservoir of the virus and an additional factor in the spread of HIV in organs and tissues. In particular, infected macrophages already at the very early stages of the disease overcome the blood-brain barrier and transfer the virus to the central nervous system and other organs. At the stage of primary infection, infection of T4 lymphocytes is accompanied by an explosive surge in viral replication (2-3 weeks from the moment of infection). This contributes to the further spread of the virus in the lymphoid organs (lymph nodes, spleen, tonsils). The number of T4 lymphocytes in the blood decreases, and the viral load (the number of copies of HIV RNA) can reach 1 million. Partial relief of acute retroviral infection is corrected by the body’s immune response mainly due to cytotoxic lymphocytes and neutralizing antibodies, detected at 3-12 weeks ( seroconversion). This is accompanied by a restoration of the number of T4 lymphocytes (but not to the initial level) and a gradual decrease in the level of viral replication (RNA concentration in peripheral blood decreases by 3-5 lg). Usually by 6-8 months. After infection, a certain plateau (setpoint) is reached in the level of replication, which reflects the balance that is achieved between the body and the virus, and the disease passes into the stage of asymptomatic chronic infection. The quantitative parameters of this balance, expressed by the number of T4 lymphocytes and the level of viral load, are individual. The term “asymptomatic” in the name of the stage refers only to clinical manifestations. Virus replication continues within the plateau; dead T4 cells are still replenished with an adequate number of new ones. Lymph nodes are overloaded with extracellular and intracellular virus, which manifests itself (but not in everyone) as persistent generalized lymphadenopathy. The duration of the reproduction cycle of one generation of the virus is 2.6 days. Half of the new virions die every 6 hours, but viremia is maintained by constant, repeated cycles of reinfection and reproduction in productively infected T4 cells. It is believed that 10 billion virions appear in the body every day, the number of virus generations per year is 140, and over 10 years more than 1400. It is calculated that any mutation at any position of the genome can occur many times a day, and with the use of drugs it can be almost any resistant mutant is generated. Duration of period clinically asymptomatic infection for 80% of patients it is 8-12 years. At the end of this period, the balance that has been maintained by the immune system for so long is disrupted. The next symptomatic phase of infection is characterized by a progressive activation of viral replication, an increase in the content of HIV RNA in the plasma, as well as a progressive increase in the destruction of the immune system, manifested in a decrease in the number of T4 cells and discoordination of many other indicators . Clinical symptoms and syndromes increase with the transition to severe progressive diseases that manifest the onset of AIDS itself. Most of these diseases manifest themselves in forms that are not found in humans with a normally functioning immune system. These diseases, which are called AIDS-defining diseases, include tumors, invasions, fungal, viral and, to a lesser extent, bacterial infections caused by opportunistic pathogens. The mechanism of immune system dysfunction in HIV infection is diverse. Cellular abnormalities are primarily associated with T4 lymphocytes. The decrease in their absolute number is determined not only by the direct cytopathic effect of the virus. One mechanism is that infected gpl20-producing cells fuse with healthy cells that have CD4 antigen in their membrane (formation of syncytia). In the same way, free gpl20 circulating in the blood can bind to CD4 molecules of undamaged cells, which are recognized by the immune system as foreign and destroyed. A hypothesis has been proposed according to which the death of T4 lymphocytes during HIV infection is associated with physiological cell death (apoptosis), triggered by the interaction of gpl20 with CD4 receptors. There are other mechanisms of HIV pathogenesis that explain the death of T4 lymphocytes. It is known that T4 lymphocytes play a central role in the regulation of the immune response, which is carried out through a system of cellular mediators-cytokines. During HIV infection, the synthesis of cytokines produced by subpopulations of T4 lymphocytes (Th-1 and Th-2) is disrupted. The secretion of IL-2 and Y-interferon, involved in the implementation of cellular immunity, continuously decreases, and IL-4 and IL-10, involved in the implementation of humoral immunity, increases. HIV-infected macrophages undergo ultrastructural changes, chemotaxis and Fc-dependent phagocytosis are disrupted . Due to the constant activation of mononuclear cells, hyperfunction of anti-inflammatory cytokines (TNF-a, IL-ip, IL-6) is observed. As a result of disturbances in the synthesis of cytokines of T-cell and macrophage origin that regulate the function of B-lymphocytes, their polyclonal activation occurs, accompanied by spontaneous production of nonspecific immunoglobulins. One of the hypotheses about the leading pathological factors in HIV infection is autoimmune pathological processes due to the cross-reactivity of a number of epitopes of viral proteins and proteins of the human body. These are just some of the many elements of the immunopathogenesis of HIV infection. In general, we can say that HIV, invading the cells of the immune system, either destroys them using various mechanisms or modifies their functions, initiating multidirectional changes in the synthesis of cytokines, which ultimately disrupts all parts of the immune system. This is the pathological basis on which the AIDS symptom complex develops. At the same time, HIV itself is exposed to the action of the immune system, since a protective response to its introduction is formed in the human body. From the very beginning of the infection, the production of specific anti-HIV antibodies begins (first Ig M, and then IgG and IgA), which persists throughout all stages of the disease with some changes in the distribution of antibodies to individual HIV proteins. However, these antibodies, at best, are only witnesses to the infection, and through a number of mechanisms they can even enhance it. Antibodies to the glycosylated form of gpl20 have virus-neutralizing properties in vitro, but do not control the development of an already established infection. One of the reasons is the high rate of virus reproduction and, as a consequence, the rapidity of involvement of more and more new cells in the pathological process. Specific antibody-dependent cellular cytotoxicity carried out by monocytes or normal killer cells in the presence of anti-HIV antibodies against cells on which HIV antigens are expressed is sufficient expressed in vitro, but the protective significance of this phenomenon has not been proven. The most important factor inhibiting HIV replication are T8 cytotoxic lymphocytes, which can directly lyse virus-containing cells or act indirectly through the cytotoxins they synthesize (CD8 antiviral factor) and (3-chemokines. It is believed that the high activity of T8 lymphocytes is the main factor in the long-term persistence of the asymptomatic infection phase in HIV-infected centenarians. In general, the answer to the key question of the pathogenesis of HIV infection - what regulates the replication of the virus - is that this role is assigned to the host body, which realized through a network of endogenous cytokines. Anti-inflammatory cytokines, indicative of chronic immune activation (TNF-a, IL-ip, IL-6) enhance HIV replication. At the same time, other cytokines, such as IL-10, IL-2, IFN-Y, CD8 antiviral factor, as well as P-chemokines inhibit HIV expression. All of these factors contribute to the balance between viral suppression and reproduction, and therefore the course of the disease. An additional role is played by numerous co-factors from the host organism, the virus, as well as concomitant opportunistic infections.Epidemiology
The source of infection is an HIV-infected person at all stages of the disease. The virus is found in blood, semen, vaginal and cervical secretions, and breast milk, which are factors in the transmission of infection. It is assumed that the infectious dose of the virus is about 10 thousand virions. Saliva, urine, tear fluid also contain the virus, but its quantity is not enough for infection. The modes of transmission are sexual, parenteral and vertical. About 85-90% of all cases of HIV infection in the world are associated with transmission of the virus through sexual contact, which allows us to attribute HIV infection is a group of sexually transmitted diseases. Moreover, on a global scale, heterosexual relationships are the cause of 70% of cases of infection, homosexual relationships - 5-10% of cases. 3-5% of HIV infections in the world are associated with infection through blood transfusions. Injecting drug users make up up to 10%, and this figure continues to increase. Vertical transmission of HIV from an infected mother to the fetus in the last months of pregnancy, at the birth of a child, or during breastfeeding in African countries it occurs in 40-50% of cases, and in economically developed countries - 25-35%. Experts believe that the intensive spread of HIV infection in the world began in the late 70s; the scale of the epidemic has been regarded as a pandemic for more than 10 years .According to WHO, at the end of April 1999, there were more than 33 million people infected with HIV and 16.3 million dead from AIDS. Currently, for every 100 people of sexually active age (15-49 years), there is one HIV carrier. In some regions, AIDS is main reason mortality among adults. Since the beginning of the AIDS pandemic, about 4.8 million children have been infected, of whom about 3.6 million have died. Sub-Saharan Africa is home to two-thirds of those infected with HIV, and heterosexual transmission of the virus dominates. In other regions of the world, the picture of the epidemic process is mixed. A typical model is the initial concentration of the virus in groups with risky behavior in relation to HIV infection (homosexuals, intravenous drug users, prostitutes), followed by the spread of the virus through their sexual partners into the general population. HIV is characterized by relatively low resistance to chemical and physical factors. Heating at 56° for 30 minutes. leads to a decrease in the infectious titer of the virus by 100-1000 times, and higher temperatures quickly and completely inactivate it. The virus quickly dies under the influence of disinfectants used in laboratory practice (70% ethyl alcohol, 3% hydrogen peroxide solution, 5% Lysol solution, 0.2% sodium hypochlorite solution, etc.). HIV, at the same time, is quite stable at room temperature in both dry and liquid environments (4-6 days), as well as to UV irradiation and ionizing radiation.HIV infection
Human immunodeficiency viruses (HIV) are members of the family Retroviridae, genus Lentivirus. There are two types of pathogens of acquired immunodeficiency syndrome - HIV-I and HIV-ILHIV-1 has a round shape, its size is 100-120 nm. The genome consists of two identical RNA plus strands associated with reversease and internal proteins. The genome contains 9 genes (3 structural: gag, pol, env and 6 non-structural: tat, rev; vift nefy vpr, vpu, encoding internal proteins of the virus, reversease, endonucleases, protease and specific proteins of the outer shell). The core of the virion is surrounded by capsid proteins and takes on a cone shape. Associated proteins are p7, p9, p24. It is separated from the outer shell by another layer of proteins - matrix (p 17). The outer lipid shell contains glycoprotein transactions consisting of two glycoprotein subunits (gp 41 and gp 120). Collectively, they are designated as gp 160. Due to the peculiarities of the genome structure, HIV has significant antigenic variability. When heated to 56 ° C for 30 minutes, the virus is inactivated. It is sensitive to the effects of alcohol, ether, acetone, ionizing and ultraviolet radiation. HIV-2 in its structure is not fundamentally different from HIV-1, but has some differences in the composition of the genome, proteins, etc.. Diagnosis of AIDS is complex and responsible . It is based on the main clinical manifestations of the disease, as well as the results of virological, serological and other research methods, and requires their comprehensive assessment.Serological diagnosis
Today, Ukraine has developed a two-stage system for laboratory diagnosis of the disease, which includes testing human blood serum for the presence of antibodies against HIV. The blood serum of persons suspected of being HIV carriers is examined using ELISA. This happens in specialized laboratories for the diagnosis of AIDS, which are deployed at the bases of SES, blood transfusion stations, clinics, dispensaries, infectious diseases hospitals, etc. The main material for research is blood. it is taken from the cubital vein in a volume of 5 ml. The serum obtained later can be stored at 4 ° C for 7 days. It is also suggested to use the image of a “dry drop”. It consists of pricking a finger with a sterile needle and applying a few drops of blood to a sterile disk made of filter paper. Dried discs can be stored for a long time (up to 6 months) in plastic bags. If necessary, using a phosphate saline solution, immunoglobulins are liquefied and tested. It has been proven that antibodies against HIV can be detected in tears, saliva, breast milk (IgA), cerebrospinal fluid (in persons with encephalopathies or neurological symptoms), even in urine . It is considered acceptable to test for the presence of antibodies in the vitreous fluid in corpses. ELISA (mostly indirect) allows you to determine antibodies in any examined material. It is a fairly sensitive method that is used in any laboratory in the world. Antigens for these test systems are obtained either from infected tissue cultures or using recombinant DNA. In Ukraine, the test systems “Antigen”, “recombinant-HIV”, “Service-HIV”, “Combi-HIV”, from Abbott and others are used. It should be noted that antibodies in the blood do not appear immediately after HIV enters the body , and no less than after 2-3 months, and sometimes longer (5-8 months). Therefore, it should be remembered that ELISA is of little use for diagnosing virus carriage during the seronegative period. A one-time positive result for detecting antibodies in the blood does not confirm the diagnosis of immunodeficiency. It is recommended to repeat this reaction three times. Two positive results in triplicate are considered diagnostic. This reaction scheme is due to the fact that modern test systems can still give both false-positive and false-negative results. Blood samples that give two positive results out of three repetitions are sent to specialized laboratories at research institutes to confirm the presence of HIV virus carriage using an enzyme-linked immunosorbent assay - Western blot or immunoblot (from English. Blot - spot), indirect immunofluorescence reaction or radioimmune precipitation. These methods make it possible to detect antibodies to certain viral proteins. The Western blot method involves preliminary electrophoretic separation of viral proteins in a polyacrylamide gel, followed by their transfer to special nitrocellulose membranes. After this, the blood samples under study are dispersed on filters, followed by identification of their proteins (antibodies against certain structural viral proteins) using anti-species labeled sera. Color stripes appear on nitrocellulose filters, corresponding to complexes formed by viral structural proteins and antibodies from the virus carrier serum. A positive result of the reaction may be indicated by the presence of antibodies against the viral proteins p24, RZI, gp41, gpl20/160. With negative results, characteristic staining zones are not visible on the filters. One of the effective ways to determine the presence of antibodies against HIV in human blood is the use of microagputation tests. It is similar to the indirect hemagglutination reaction, but instead of erythrocytes sensitized with the corresponding antigen, gelatin or latex particles are used as the basis. In case of a positive result, observe the appearance of a specific precipitate in the wells of the plate. This reaction gives similar results to ELISA, however, it is much simpler in terms of the procedure, is faster to perform, and gives fewer false-positive results. Another method for detecting antibodies against HIV is the indirect immunofluorescence reaction. To stage this reaction, an antigen is used, which is obtained from continuous lines of lymphocytes infected with immunodeficiency viruses. Fixed cell preparations are prepared from them, which can be stored for 2 months at a temperature of -20 ° C. If necessary, glasses with applied antigen are treated with diluted test sera (1:10, 1:100, 1:1000, etc.), and then with fluorescent antiserum against human immunoglobulins. The preparations are additionally contrasted with Evans blue and examined under a fluorescence microscope. The radioimmunoprecipitation method is more sensitive. As with any immunological reaction, it is based on the interaction of HIV antigens with antibodies against them. In this reaction, HIV proteins labeled with radioactive isotopes 125I or 35S are used as antigens. The reaction is carried out in the liquid phase, mixing homologous antigens (viral proteins gpl20, gp41, p24, p17, p9 and others) and antibodies (virus carrier serum), resulting in the formation immune complexes. They interact with a special system, which consists of S. aureus protein A connected to sepharose, resulting in precipitation. The resulting complex is precipitated in test tubes using ultracentrifugation, the supernatant is removed, leaving only the antigen-antibody-protein A-Sepharose substrate. At the next stage of the study, the complexes are dissociated with sodium dodecyl sulfate, subjected to electrophoresis in a polyacrylamide gel, and the molecular weight of isotope-labeled proteins is determined using autoradiography. This makes it possible to determine which viral proteins are located in immune complexes, and therefore to which viral proteins antibodies are formed. This method is more sensitive than immunoblotting, but requires special equipment, so it is not widely used in laboratory practice. To summarize, this is how we can approach confirmation of the diagnosis of HIV carriage. A one-time negative result for the presence of antibodies obtained using ELISA allows us to conclude that there is no HIV infection. Two positive results from three repeated sera tests do not allow a diagnosis of virus carriage to be made. This can only be done after positive results for the presence of antibodies against certain viral structural proteins using immunoblotting or other methods, it is replaced.Virological diagnostics
The material for research can be blood, cerebrospinal fluid, breast milk, sperm, autopsy biopsies, etc. To identify the virus, electron microscopy is used to infect cultures of T lymphocytes (CD4 cells). To identify viruses, it is possible to use highly sensitive ELISA test systems, indirect immunofluorescence reactions, which have a similar cytopathic effect. Important for the diagnosis of AIDS is the determination of the provirus in lymphocytes, or viral nucleic acids in pathological material. For this purpose, molecular hybridization methods are widely used. The use of this method becomes important especially due to the fact that the seronegative period for AIDS can last several months. The high sensitivity of the proposed method makes it possible to detect even single viral particles in the blood (0.1-1.0 ng of nucleic acids). Its principle is that, under in vitro conditions, a process of hybridization is caused between the viral nucleic acid (DNA, RNA) and a special probe, which is labeled with radioactive phosphorus 32P. The resulting complex is quite easy to identify using autoradiography. However, the use of 32P probes complicates this method to a certain extent, since they have a short (2 weeks) half-life and require strict safety regulations when working with radioactive isotopes. Taking this into account, a promising direction is the use of probes that can be detected using color enzymatic reactions. Such a label is biotin (biotin probe). There are various options molecular hybridization, among which dot hybridization, blot hybridization, sandwich hybridization, and in situ hybridization (in infected tissues) are most often used. One of the options for molecular hybridization is the polymerase chain reaction, which is based on gene amplification. The use of DNA polymerase, for example, with Thermophylus aquaticus, allows for several amplification cycles to significantly increase the number of studied nucleic acids, as a result of which they can be detected by any known methods - ELISA, polyacrylamide gel electrophoresis, etc. This reaction significantly exceeds the sensitivity of the previous method (by several orders of magnitude), and therefore can be used in the study of microvolumes of material or test objects where immunodeficiency viruses are not detected by other methods, for example, nasopharyngeal swabs, saliva. In addition to the described diagnostic methods, it is considered acceptable detection of antigenemia, which is caused by the p24 protein. This p24 antigen can be determined using modified ELISA methods. Obtaining a positive result when using one of the following methods is a sufficient argument for establishing the etiological diagnosis of HIV infection. Virological diagnosis of AIDS is a rather complex process that can only be performed in highly specialized laboratories where all necessary conditions for work (protection of personnel from infection during the cultivation, purification and concentration of HIV) and are highly qualified specialists. Thus, in the presence of HIV infection in virus carriers or patients with AIDS, the following virus-specific markers can be detected: antibodies to HIV, the infectious virus itself , provirus in the DNA of affected immunocytes, viral antigen in blood serum and infected target cells.The abbreviation HIV stands for human immunodeficiency virus. This virus is the main cause of acquired insufficiency of the functional activity of the immune system, namely its cellular component. Today, this infection is very common and tends to further increase the number of infections.
HIV virus, types and properties
The human immunodeficiency virus is a retrovirus and belongs to the lentivirus genus. This is an RNA virus, its main feature is the process of reverse transcription. This means that when it enters a cell, the RNA molecule of the virus, under the influence of the enzyme reverse transcriptase (revertase), is converted into DNA, which is integrated into the genome. During its life, a cell with viral DNA in its genome begins to synthesize new RNA and viral capsules that come out of it and infect new cells.
Moreover, the built-in section of viral DNA remains in the cell forever, does not manifest itself for a long time and does not lead to its death. This feature determines that HIV is a slow infection, with the progression of the infectious process over a long period (at least 10 years). The main distinguishing property of HIV is selectivity. It is capable of infecting cells that have specific CD 4 receptors on their surface, which are contained in immune cells - T-lymphocytes, dendritic cells (perform protective functions in the tissues of the nervous system), tissue macrophages. Over time, infected cells lose the ability to perform their main biological function - supporting the cellular component of immunity. There are 2 types of immunodeficiency virus:
- Type 1 - distributed on all continents.
- Type 2 - found mainly in Central African countries.
The immunodeficiency virus has a complex structure. Its genetic material, RNA, is covered by a protein capsule that  covered with a layer of phospholipids (supercapsid). Inside the viral capsule is the enzyme transcriptase, which catalyzes the process of converting viral RNA into DNA inside the cell. In the external environment, HIV is unstable and quickly dies under the influence of high and low temperatures, sunlight, and disinfectant solutions (hydrogen peroxide, bleach, alcohol).
covered with a layer of phospholipids (supercapsid). Inside the viral capsule is the enzyme transcriptase, which catalyzes the process of converting viral RNA into DNA inside the cell. In the external environment, HIV is unstable and quickly dies under the influence of high and low temperatures, sunlight, and disinfectant solutions (hydrogen peroxide, bleach, alcohol).
The discovery of the virus dates back to 1981, it was discovered in Africa. Today, there are several hypotheses for its appearance - the impact on a non-pathogenic virus of a precursor of an unfavorable environment with its subsequent mutation into HIV, the formation of the virus during the development of biological weapons. Mutation of the virus under the influence of radiation, which is increased in some African countries due to the large amount of uranium ores, the origin of HIV is from the simian immunodeficiency virus. All of these hypotheses attempt to explain the lack of mention of a disease similar to AIDS throughout human history.
What is HIV AIDS
HIV infection is an infection with an immunodeficiency virus without the development of an underlying disease. The state of HIV infection can last quite a long time, without any clinical manifestations. AIDS is a syndrome of acquired immune deficiency (immunodeficiency), it develops in the midst of an infection and is characterized by damage to a significant number of immunocompetent cells (macrophages, lymphocytes). Signs of AIDS include a decrease in the activity of the immune system, which is manifested by the development of diseases caused by representatives of opportunistic flora or other pathogens that the immune system normally suppresses (opportunistic infections). Such infections include:
- Candidiasis (thrush) caused by an opportunistic fungus of the genus Candida.
- Cytomegalovirus infection.
- An infectious process caused by the Epstein-Barr virus.
- Skin lesions (multiple pustules).
- Pneumocystis pneumonia.
HIV and AIDS, the difference lies precisely in the presence of decreased immunity and the development of opportunistic infections and other pathologies associated with immunodeficiency (oncological process).
How do you get infected with HIV?
The immunodeficiency virus is a parenteral infection. Ways of contracting HIV infection include:
- Sexual transmission - the virus enters the body of a healthy person through direct contact of the mucous membranes of the genital organs with an infected partner. Moreover, the risk of infection is higher for the receiving party, so women become infected more often during classical sexual intercourse. The risk is even higher when engaging in anal sex, since additional microdamage to the rectal mucosa occurs. Oral sex is safer; infection is possible only in the presence of injuries or erosions of the oral mucosa.
- The virus enters the bloodstream through a syringe when using injecting drugs.
- Infection during various medical procedures and manipulations involving violation of the integrity of the skin or mucous membranes with undisinfected instruments.
- Transfusion of contaminated blood or its components.
- Vertical transmission - the virus is transmitted from an infected mother to the fetus during pregnancy (less often) or the child is infected during childbirth and subsequent breastfeeding.
 The transmission factor for HIV is human biological fluids - semen, breast milk, vaginal secretions, blood. The virus is not released in human saliva. The source of infection is a sick person (AIDS) or a virus carrier (HIV-infected).
The transmission factor for HIV is human biological fluids - semen, breast milk, vaginal secretions, blood. The virus is not released in human saliva. The source of infection is a sick person (AIDS) or a virus carrier (HIV-infected).
The development of disposable sterile medical instruments was dictated by the need to minimize the possibility of HIV infection during various medical procedures.
Probability of infection
The main condition that promotes infection is the number of viral particles in the biological fluid with which the human internal environment has come into contact. Transmission routes also influence the likelihood of infection:
|
Transmission path |
Probability of infection |
|
Anal sex |
1% for the receiving party |
|
Vaginal sex |
0.1% for women, 0.01% for men |
|
Vertical path (from mother to child) |
|
|
Contaminated blood transfusion |
|
|
Injecting drugs with a contaminated syringe |
Using condoms minimizes HIV transmission. They also protect against other sexually transmitted infections - viral hepatitis B and C, syphilis, gonorrhea, chlamydia, ureaplasmosis.
Symptoms of HIV
HIV does not show itself for a long time. The period from the moment of infection to the development of AIDS lasts from 5 to 20 years. When a large number of viral particles enter the human body, a clinical manifestation of the body’s primary reaction is possible. It develops 1-3 weeks from the moment of infection,  characterized by a rise in temperature, enlarged lymph nodes, and unstable stools. Usually these phenomena go away on their own within a few days. From this moment on, the virus is already introduced into immune cells and remains in them for a long time, without showing itself in any way. These primary symptoms of HIV occur in the same way in women and men. That is why laboratory diagnosis of HIV infection is very important, which consists of determining antibodies in the blood to the virus and its genetic material in the body.
characterized by a rise in temperature, enlarged lymph nodes, and unstable stools. Usually these phenomena go away on their own within a few days. From this moment on, the virus is already introduced into immune cells and remains in them for a long time, without showing itself in any way. These primary symptoms of HIV occur in the same way in women and men. That is why laboratory diagnosis of HIV infection is very important, which consists of determining antibodies in the blood to the virus and its genetic material in the body.